Given that this is a holiday weekend, I had been considering taking a week off to hang out, go on long bike rides, and do some yard work. Then—wouldn’t you know it?—on Thursday, the Trump administration and his “make America healthy again” (MAHA) antivax crank and toady, Robert F. Kennedy, Jr., dropped The MAHA Report, with a press release filled with the typical hyperbole and self-congratulatory wankery that we’ve come to know and hate about RFK Jr.:
The Presidential Commission to Make America Healthy Again (MAHA) today released a groundbreaking assessment identifying key drivers behind the childhood chronic disease crisis. Coming just 98 days after President Trump signed an Executive Order, links to an external website establishing the MAHA Commission and tasking it with delivering a “Make Our Children Healthy Again Assessment, links to an external website,” the report exposes a range of contributing factors—including poor diet, accumulation of environmental toxins, insufficient physical activity, chronic stress, and overmedicalization.
By examining these drivers, the assessment arms MAHA Commission stakeholders and partners with clear evidence that will support the development of effective policy interventions where they can deliver the greatest impact.
“We will end the childhood chronic disease crisis by attacking its root causes head-on—not just managing its symptoms,” said U.S. Health and Human Services Secretary Robert F. Kennedy, Jr. “We will follow the truth wherever it leads, uphold rigorous science, and drive bold policies that put the health, development, and future of every child first. I’m grateful to President Trump for his leadership—and for trusting me to lead this fight to root out corruption, restore scientific integrity, and reclaim the health of our children.”
I debated not writing anyway, but, me being me, I couldn’t resist this big fat juicy target dropped in front of me, even if I didn’t become aware of it until Friday morning, thanks to a long day in clinic on Thursday followed by attending to family business in the evening. Also, I had already discussed the executive order forming the MAHA Commission, the committee tasked with writing this report in February. As I discussed then, the EO was full of health misinformation about cancer, autism, and ADHD just by itself; so I wanted to see what the final product ended up saying. Let’s just say, it’s a mixture of The Good (very little but not nonexistent), The Bad and The Ugly (the vast majority of the report.)
So let’s take a look at the report. I’ll start with its introduction, which is, predictably, full of RFK Jr.-inspired false premises. Then we’ll look at The Good (which is invariably contaminated with The Bad and the Ugly), and then The Bad and The Ugly, discussion of which will take up the bulk of this post.
Membership
Any time one analyzes a report by a commission or a committee, it’s important to look at who the members are, as who the members are will shape the report. So I perused the list of members. Of course, RFK Jr. chaired the commission, as was expected based on the executive order.
What really struck me, however, was how few of the commission members have any expertise in medicine. For example, the only two members of the commission trained in medicine are FDA Commissioner Dr. Marty Makary and NIH Director Dr. Jayanta (“Jay”) Bhattacharya, the latter of whom never completed a residency and has never practiced medicine since medical school. Dr. Makary is best known for being a COVID-19 minimizer and anti-COVID-19 vaccination, as well as, pre-pandemic, for having created the myth in 2016 that the third leading cause of death in the US is medical error, basically putting a faux legitimate face on longtime quack myths about “death by medicine.” Dr. Bhattacharya, of course, was one of the authors of the Great Barrington Declaration, the October 2020 manifesto that proposed opening up society from “lockdowns” (which were largely already disappearing then anyway) through a “let ‘er rip” approach to the pandemic, with a poorly articulated afterthought of “focused protection” of those at high risk for severe disease and death from COVID-19, specifically the elderly and those with certain chronic medical conditions. Bhattacharya was well known for his consistently wrong repeated claim that this approach would bring natural herd immunity in 3-6 months, a claim that Makary was totally happy to parrot. In other words, they’re both down with the soft eugenics of MAHA.
The rest of the membership show little evidence of anything resembling expertise in the subject areas necessary to “make America healthy again.” Stephen Miller? Seriously? He’s known for his xenophobia and anti-immigration stances, rather than any expertise in public health. Linda McMahon? She’s a former professional wrestling promoter and entrepreneur turned Secretary of Education. Michael Kratsios? He’s a former businessman turned political operative. Russell Vought? He’s the Director of the Office of Management and Budget and believed to be more the one behind all the budget cuts at HHS, as well as the defunding of so many previously awarded NIH research grants. Worse, he’s someone whose child benefited from NIH research but who has since being appointed OMB Director mercilessly hacked away at the NIH budget. Then, of course, many of the members have purviews in economic policy, rather than in medicine, research, public health, or science.
A less competent group of individuals to “make America healthy again” is hard to imagine, at least for me. I fear that it probably isn’t hard for RFK Jr. or Donald Trump to imagine.

Glorious purpose
If there’s one thing about MAHA (and MAGA in general), it’s that its adherents can’t seem to view their mission with anything less than apocalyptic Manichaeism, and good vs. evil dualism in which the triumph of evil would mean the end of everything good and our children being doomed to unhealth forever. Here’s an example from the statement of purpose:
It presents the stark reality of American children’s declining health, backed by compelling data and long-term trends. More importantly, it seeks to unpack the potential dietary, behavioral, medical, and environmental drivers behind this crisis. By examining the root causes of deteriorating child health, this assessment establishes a clear, evidence-based foundation for the policy interventions, institutional reforms, and societal shifts needed to reverse course.
To turn the tide and better protect our children, the United States must act decisively. During this administration, we will begin reversing the childhood chronic disease crisis by confronting its root causes—not just its symptoms. This means pursuing truth, embracing science, and enacting progrowth policies and innovations to restore children’s health. Today’s children are tomorrow’s workforce, caregivers, and leaders—we can no longer afford to ignore this crisis.
After a century of costly and ineffective approaches, the federal government will lead a coordinated transformation of our food, health, and scientific systems. This strategic realignment will ensure that all Americans—today and in the future—live longer, healthier lives, supported by systems that prioritize prevention, wellbeing, and resilience.
I can’t help but notice a number of things. First, notice the emphasis on how “today’s children are tomorrow’s workforce.” Sound familiar? It’s just a softer version of what RFK Jr. said about severely autistic children, namely that they will never pay taxes, hold a job, get married, or play baseball. In other words, it’s a “kinder, gentler” statement of “useless eater” rhetoric to describe chronically ill children and is basically eugenicist. Am I being unfair? You might convince me of that if this were the only statement like this from MAHA leaders, but it’s simply another restatement of the same narrative, watered down to make its eugenicist tendency less apparent. Also, don’t get me wrong. No one—and I mean, no one wants children to suffer from chronic illnesses and health conditions. We just differ on what the reasons behind childhood chronic illness are, as well as the scope of the problem, which RFK Jr. has been exaggerating and misrepresenting ever since his antivax org Children’s Health Defense came up with the narrative of this generation being the “sickest children.” (Hint: As I have explained, they are not.)
The Good, The Bad, and The Ugly
As I mentioned above, there are some reasonable parts to the MAHA Report, but unfortunately even those good parts tend to be contaminated with exaggerated and/or pseudoscientific MAHA narratives. In the introduction, The MAHA Report, predictably, identifies four key problems responsible for this “crisis” of child health, which sounds suspiciously like the language of the “sickest generation.” Indeed, in the introduction, The MAHA Report even states:
Today’s children are the sickest generation in American history in terms of chronic disease and these preventable trends continue to worsen each year, posing a threat to our nation’s health, economy, and military readiness.
There goes the “soft eugenicist language” again. I note that the reference cited to support the claim that today’s children represent the “sickest generation” is this one, which does report that the percentage of children with chronic conditions or functional limitations has increased from 22.6% to 30.2% from 1999/2000 to 2017/2018, as reported by the National Health Interview Survey. Of course, as I noted when I first addressed the “sickest generation” trope, this survey likely undercounted many conditions in the past. For the moment, though, let’s accept that we have a problem with chronic disease in our children, which is undeniable. What would a science-based approach to addressing the problem look like? Hint: Not like what The MAHA Report advocates.
Let’s start with the four main problems identified in the report:
- Poor diet
- Aggregation of environmental chemicals
- Lack of physical activity and chronic stress
- Overmedicalization
Right from the start, you can see the way that MAHA characteristically takes a germ of truth and then throws in a lot of its usual nonsense. For example, there is little doubt that many children suffer from poor diet and lack of physical activity. Addressing those problems is undoubted worthwhile, but it depends on how that is done. Similarly, overmedicalization can in some instances be a problem, but, as you will see, part of The Bad and The Ugly is how MAHA is basically anti-psychiatry and wants discourage the use of psychiatric medications even when appropriate, as for depression, anxiety, and ADHD. Much worse, as you will see, MAHA includes the childhood vaccination schedule under “overmedicalization,” parroting the antivax narrative that the expansion of the childhood vaccine schedule since the 1990s as the cause of neurdevelopmental conditions and chronic disease. Indeed, there is a long section on the childhood vaccine schedule, full of common antivax tropes that RFK Jr. has long been promoting. Many of the tropes will be very familiar to regular readers. In addition, the report also includes under “overmedicalization” gender-affirming care of children with gender dysphoria and trans adolescents, which is described in unscientific terms, such as “child chemical and surgical mutilation.”
The MAHA Report plays the same game with environmental chemical exposures. For example, it includes examples of chemical exposures for which there is sufficient scientific evidence to be concerned about a possible health impact from exposure, particularly in children, such as microplastics, PFAS, biphosphenols, and the like. Fair enough, even if the cases as presented are one-sided. To this, The MAHA Report adds fluoride, which is safe at the doses and exposures used in drinking water and fluoride products, while ignoring the benefits to dental health that come from fluoridated water and the use of fluoridated dental products. It also includes, predictably, pesticides, especially glyphosate, which is safe at the exposures users experience and is mainly a concern in agricultural workers exposed to much higher amounts of it.
And get a load of what The MAHA Report says about electromagnetic radiation (EMR):
…an exposure due to the proliferation of cell phones286, Wi- Fi routers, cell towers, and wearables)287 Some studies have linked EMR exposure to reduced sperm counts and motility but not quality.288 The NIH’s National Toxicology Program identified “clear evidence” of DNA damage and increased cancer risk in rats.289 However, a recent systematic review of over 50 studies found low to inadequate evidence on impact in children and called for more high-quality research.290
We have written about the various overblown claims that EMR contributes to cancer going back decades (most recently Steve Novella wrote about it in 2024), and I have specifically written about the awful study that claimed to show that EMR caused cancer in rats and its many deficiencies. Let’s just say that RFK Jr. is being RFK Jr., mixing concerns about poor diet and sedentary lifestyle with overblown and unsupported claims about fluoride, vaccines, and the like.
Also tellingly, as others have pointed out, key drivers of poor health, disability, and death among children are conveniently left out:
But as a governmental, “scientific” document, it omits some of the most common causes of chronic disease and death among children, notably car crashes and gunfire, the leading causes of death among young Americans. It never mentions teenage smoking and alcohol or drug use. Or access to physical or mental health care. It prefers to criticize fluoride in drinking water (without discussing its beneficial effects) than to take on less popular or profitable targets like guns and social striations.
As I like to note, if you want children to eat healthier, you need to address inequalities that lead large numbers of children to lack access to healthy food. You need to address food deserts. Yet, nowhere in the report is any discussion of how to address this problem. Instead, there is a section discussing the food pyramid, even though the food pyramid was phased out by 2011 and hasn’t been a thing as far as food recommendations go for a long time. Again, the part on foods mixes the reasonable with the not-so-reasonable coupled with convenient omissions, such as how it discusses how industry has influenced the Dietary Guidelines for Americans (DGA). These issues are discussed with respect to government food assistance programs, such as Supplemental Nutrition Assistance Program (SNAP, formerly known as food stamps), the School Breakfast Program and National School Lunch Program (NSLP), and the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC), the latter of which is praised as having a “proven track record for improving children’s health.”
Of course, if RFK Jr. wants to wield the power of the federal government to encourage healthy eating, it is puzzling that the Trump administration is proposing massive cuts to all of the above programs, including massive cuts to SNAP and WIC.
And vaccines. Oh, yes, The MAHA Report is antivaccine.
MAHA vs. vaccines
I’m going to start by extensively quoting the section on childhood vaccines:
Vaccines benefit children by protecting them from infectious diseases. But, as with any medicine, vaccines can have side effects that must be balanced against their benefits. Parents should be fully informed of the benefits and risks of vaccines. Many of them have concerns about the appropriate use of vaccines and their possible role in the growing childhood chronic disease crisis.
- Since 1986, for the average child, by one year of age, the number of recommended vaccines on the CDC childhood schedule has increased from 3 injections to 29 injections (including in utero exposures from vaccines administered to the mother). Of course, parents may choose to delay to a later age or forego one or more of these vaccines.454 455
- The number of vaccinations on the American vaccine schedule exceeds the number of vaccinations on many European schedules, including Denmark, which has nearly half as many as the U.S.456 457 458 Yet, no trials have compared the advisability and safety of the U.S. vaccine schedule as compared to other nations.459
- Unlike other pharmaceutical products, vaccines are unique in that all 50 states enforce some form of vaccine mandate for public school enrollment although almost all states allow exemptions for religious and/or personal reasons.460 In contrast, over half of European countries—including the UK—do not require childhood vaccination.461
Despite the growth of the childhood vaccine schedule, there has been limited scientific inquiry into the links between vaccines and chronic disease, the impacts of vaccine injury, and conflicts of interest in the development of the vaccine schedule.
Sound familiar? These are basically the “too many too soon” trope beloved of antivaxxers at least since Jenny McCarthy, as well as the implication that childhood vaccine schedules are not evidence-based because they differ among nations. As I wrote nine years ago, childhood vaccination schedules vary among nations because different diseases are more prevalent in different countries and different healthcare considerations come into play. None of that means that the vaccine schedules recommended, by, say, European countries are more or less evidence-based than the vaccination schedule recommended by our CDC. There are more than one evidence-based way to skin the proverbial cat, so to speak, and different countries choose different strategies based on the local relative burdens of different vaccine-preventable diseases. Moreover, as Dr. Vincent Iannelli pointed out in 2017, our vaccine schedule has been pretty similar to those of other industrialized countries, including European countries and Asian countries like Japan. He does describe some differences, but the differences are not always in favor of fewer vaccines or fewer doses of vaccines, for instance:
And in many European countries, even if you don’t get more vaccines overall, you do get more dosages at an earlier age, often with two dosages of MMR and the chicken pox vaccine by the time your child is 15 to 24 months old.
Some vaccines, like hepatitis A and chicken pox aren’t routine in every European country, like Iceland and Sweden, but many countries give vaccines that we don’t, like BCG and MenC. And even Iceland and Sweden have recently added the HPV vaccine to their schedule and Sweden may soon add the rotavirus vaccine too.
Again, as I said, there are more than one evidence-based strategies to protect one’s children against vaccine-preventable diseases, and they need to be tailored to the diseases for which the population is at risk. You’d think MAHA, being all about “individualization and personalization,” would be all about that, but you’d be wrong. As Dr. Iannelli adds, some European countries “give more vaccines by 12 months because they also give meningococcal vaccines to infants!”
As for “too many too soon,”The MAHA Report claims, for instance:
Since 1986, for the average child, by one year of age, the number of recommended vaccines on the CDC childhood schedule has increased from 3 injections to 29 injections (including in utero exposures from vaccines administered to the mother). Of course, parents may choose to delay to a later age or forego one or more of these vaccines.454 455
Once again, Dr. Iannelli explains why this is deceptive, not the least because the inclusion of only injections before the age of one in 1986 left out the oral polio vaccine (two doses) and pushes the MMR injection out of that one year mark, given that in 1986 the MMR wasn’t given until 15 months. At the same time, to get to 29 injections before the age of one, The MAHA Report, well, lies:
Infants do not get 29 injections, even if you include all the recommended doses that can be given to their mothers when they are pregnant.
To get to 29 injections, the MAHA folks are including the oral rotavirus vaccines (not an injection!) and are doubling up on the RSV vaccine (either mom or baby get vaccinated, not both). They are also including all the vaccines that infants could get after they are a year old, and they are going with the maximum doses possible.
And since that still only gets you to 28, they must also be including the baby’s vitamin K shot, something they would also have gotten in 1986!
So how many injections do infants really get?
You can see from the immunization schedule above that they can get as few as 17 injections, including RSV, flu, and COVID shots by the time they are 12 months old. Add in three more if mom got Tdap, flu, and COVID.
Moving on from the above trope, I almost hate to have to repeat this so often, but the call for “clinical trials” of different countries’ vaccination schedules ignores all that and represents “methodolatry” or, as I also call it, evidence-based medicine fundamentalism being weaponized to undermine confidence in the vaccine schedule. The MAHA Report even trots out the “no saline placebo” trope that falsely insinuates that the childhood vaccination schedule is unsafe because some of the vaccines have never been tested against saline placebo. It’s a trope that ignores medical ethics, which say that it’s unethical to test a second or subsequent generation vaccine against placebo if a safe and effective vaccine already exists; in such cases, the new vaccine is tested against the existing vaccine.
As for the related claims that vaccines undergo small trials and limited safety monitoring, Dorit Rubinstein included a link to a listing of why that is not true:
In particular, there is this list of pre-licensure clinical trials of various vaccines:
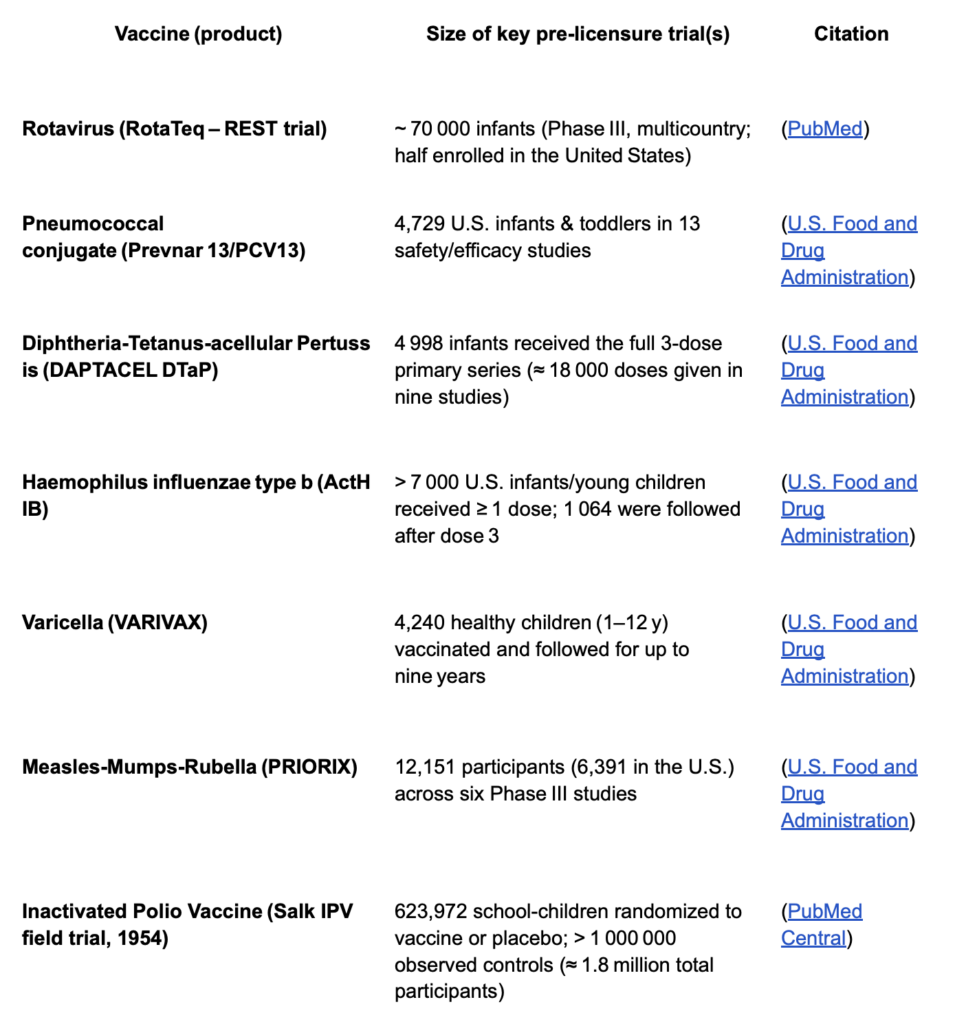
You get the idea.
The MAHA Report also trots out familiar antivax attacks on vaccine safety monitoring systems, including the Vaccine Adverse Events Reporting System (VAERS) and the Vaccine Safety Datalink (VSD). I won’t go into those in more depth here, as I have discussed such tropes more times than I can remember (particularly about VAERS), but readers will recognize the tropes, should they decide to read the relevant section.
Corporate capture vs…what?
Another key disconnect that I see in The MAHA Report is a lot of discussion of corporate capture. Again, this is an example of how RFK Jr. takes legitimate concerns about science, medicine, and the pharmaceutical industry and weaponizes them to his antivax, anti-psychiatry agenda. For example, it is not antivax or anti-psychiatry to question industry influence on regulatory bodies. However, The MAHA Report goes far beyond that, for example::
In the United States, private industry funds five times as many clinical trials than all U.S. Federal agencies combined including the NIH.479 Since 1999, 97% of the most frequently cited clinical trials received funding from industry480 The number of citations is a measure of papers’ impact,481 suggesting nearly all of the most impactful clinical trials have been funded by industry.
Let me just play Devil’s advocate for a moment and, for the purposes of argument, accept these figures. What should be done, if the above were true. Certainly one obvious response to this problem would be public funding of clinical trials used for drug approval, and the NIH would be the institution perfectly suited to fund such trials, either intramural (inside the NIH) or by funding independent investigators through external grants to carry out such trials. Alternatively, the FDA could require that industry pay for all or part of the necessary clinical trials but pick independent investigators to carry them out. That must be why the Trump administration budget proposal for FY2026 includes a massive 40% cut to the NIH budget and a 5.5% cut to the FDA budget. One also can’t help but note that all the concern about environmental chemicals, both where warranted and where unwarranted seems not to have filtered up to actual budgetary policy. After all, the Environmental Protection Agency is facing a 55% budget cut for FY2026, while the CDC, which also investigates environmental contributions to disease and chronic diseases, is facing a budget cut of one-third.
As for The MAHA Report’s critique of the use of psychiatric meds, even though it echoes concerns that some physicians and psychiatrists have expressed, let me just cite Eric Reinhart, who wrote in February about RFK Jr.’s Mental Health Bait and Switch, in particular the contrast between what physicians practicing evidence-based medicine and research and RFK Jr. when it comes to concerns about the number of people (including children) on psychiatric medications:
Despite the superficial resonance between MAHA and progressive critiques of psychiatry, the differences between them could not be more pronounced—nor more consequential. And an untold number of patients could get ground up in the gears of these distinctions.
Today, roughly a quarter of all U.S. adults take at least one prescribed psychiatric medication—a massive increase compared to prior decades, even as there have been no notable improvements in the effectiveness of available treatments, which remain disappointingly limited. Meanwhile, rates of death by suicide, overdose, and alcohol continue to increase, with a striking 37 percent increase in suicide rates between 2000 and 2018—the same period in which rates of antidepressant use in the U.S. more than doubled. Clearly, psychiatric diagnoses and treatments are—by themselves—woefully inadequate responses to the sea of psychic suffering and accompanying nihilism plaguing American society.
Social and critical psychiatry respond to this reality by demanding investments in public systems for nonmedical social care that are significant enough to prevent much of the current need for psychiatrists and psychiatric drugs. Trump and Kennedy, by contrast, respond to it by seeking to dismantle public care systems altogether, plotting major cuts to Medicaid, the Indian Health Service, food assistance, and a plethora of other essential programs that threaten to leave those in greatest need with nothing at all. This is a strategy to abandon the most exploited members of our society, exacerbating their suffering and hastening their premature deaths.
Put bluntly, the MAHA agenda—irrespective of the varying intentions of its supporters, who include millions of diverse people failed by our current systems—is quickly being turned by the Trump administration into a eugenics campaign in the guise of reform: a cynical strategy to grant symbolic recognition of widespread pain and anger at failing U.S. mental health care as a perverse means of enabling material redistribution of resources away from redress of that suffering and instead into the pockets of the rich.
The MAHA Report is the policy embodiment of this contrast. It cherry picks statistics and seems to take an attitude that treating mental illness is a matter of will that can be accomplished without drugs, while deceptively emphasizing that a lot of psychiatric drugs are prescribed “off-label” in children, neglecting to mention the reasons. If you read the American Academy of Child & Adolescent Psychiatry statement on off-label prescribing, you’ll see that there are a number of quite scientifically defensible reasons why psychiatric meds are so often used off-label in children, stating:
Off-label medication use is part of the standard of care in the treatment of psychiatric disorders when: 1) there is a solid evidence base for the medication; 2) an off-label medication has better efficacy and/or safety evidence than an on-label one; 3) a child has symptoms that are not controlled by, or experiences unacceptable side effects due to, an on-label medication; 4) a child has a disorder or comorbid conditions for which there is no FDA-approved treatment; 5) adjunct medication is necessary for control of side effects of another medication; and/or 6) a child is below the age for which an FDA approved treatment is available.
Notice how that doesn’t sound nearly as scary as RFK Jr. makes it sound or The MAHA Report portrays it. That’s not to say that overprescribing of psychiatric medications isn’t a problem that should be addressed, but what The MAHA Report implies echoes the same sorts of anti-psychiatry tropes spread by Scientology. The situation is much more complicated, with some medications being arguably overprescribed, while others are arguably underprescribed.
Gold Standard Science?
Of all the catchphrases and buzzwords to have come out of the Trump administration, “gold standard science” and its variants are among the most annoying; so naturally The MAHA Report ends with a section entitled Next Steps – Supporting Gold-Standard Scientific Research and Developing a Comprehensive Strategy. There, we see:

All of these are a mix of scientifically valid with the dubious. For example, I’m not sure what the heck they’re talking about regarding post-marketing surveillance here. We already do post-marketing surveillance, particularly for vaccines. As for the replication crisis, I’ve long said that this was always an overblown “crisis.” As I like to say, there is a reproducibility problem, but it’s not a crisis, and there are many reasons for it, and Steve Novella has written more nuanced discussions on the issue, noting that the “problem with findings that don’t replicate is not that the original study was a false positive, or the new hypothesis was wrong,” adding that “these are unavoidable and part of the scientific process.” My concern is less with the ten potential “solutions” to the problems identified in The MAHA Report but rather how they will likely be used.
Leave it to RFK Jr.’s boss President Donald Trump to sign an executive order entitled Restoring Gold Standard Science on the day after The MAHA Report was released. Declaring that “for too long, bureaucratic agendas, political interference, and inconsistent standards have eroded the American people’s trust in science,” Trump proclaims that this administration will use only “gold standard science.” Basically, the declaration expands the concept of “gold standard science” to all sciences, not just biomedical sciences, and he misrepresents evidence in other areas, such as climate science and environmental science, with a clear bias towards promoting fossil fuels and more fishing. Don’t believe me? Read the Fact Sheet associated with the EO.
Of course, any term like “gold standard science” coming from this administration clearly means science the way we want it, slanted to our ideological ends. As vaccinologist and pediatrician Dr. Peter Hotez put it:
My view: this is gaslighting, implying that before science wasn’t conducted at the highest “gold
standard” but somehow RFK Jr’s pseudoscience based on a highly corrupt health and influencer industry will fix everything with their “appropriate” science. Lysenko said much
the same.
I’ve been saying that, with this administration in general and RFK Jr. in charge of HHS in particular, Lysenko 2.0 is here. It’s called MAHA, and it won’t make America healthy again. It’s a con.


, but mostly the bad and the ugly (a lot).){kind=link}